Dr Frame’s crucial case notes | ACL and medial meniscus injury


Oh the excitement of waking up and realising you are just a shower and a croissant away from setting off on the first day of that ski holiday you’ve been planning for months. Make sure it’s a good one. Not like my best mate, who looks more nervous than excited when he recalls last year’s trip… We’re not allowed to talk about it, but I can tell you guys in the hope that you don’t end up enduring the same fate.
For the purposes of this, we’ll call him George. George is a good skier, and we’ve skied much of the Alps together. He did, however, have an unfortunate incident that was not his fault. We’ve all been in the situation where we’ve tensed every muscle in anticipation of total annihilation as we hear that noise of an out-of-control skier straight-lining it down an icy red, about to collect the orange ‘LANGSAM/RALENTIR’ sign like a runner winning the 100m.
The only problem was that this particular chap missed the orange sign, and George was the target. He was launched into the netting and, after the dust settled, appeared hobbling and bewildered. In a split second, his ski holiday was done.
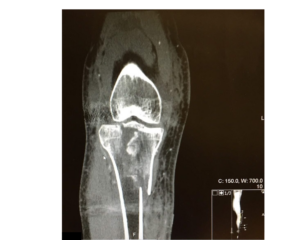
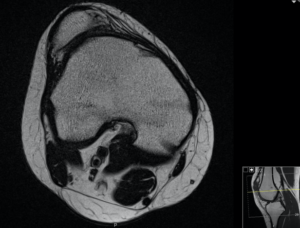
Eventually, George made it home and into the office of his local orthopaedic surgeon. One MRI scan later, he was shown to have an injury to his anterior cruciate ligament (ACL) and his medial meniscus (the disk of cartilage between the knee).
It was not the norm though. The meniscal tear had flipped, locking his knee – a ‘bucket handle tear’ – preventing him from fully straightening it, and the ACL, rather than tearing, had pulled off the tibial (shin bone) side with a small chunk of bone.
Although nasty, both injuries could be repaired. The key was speed, as they needed to be dealt with sharpish, ideally within three weeks. George had his surgery and did well with his rehab. A year on, he’s back and ready to go again.
The meniscus is so important for the functioning of your knee, and any injury that can be repaired is best given that opportunity. We can do this all keyhole, with small stitches that hold the disk of cartilage back in place until it heals. The ACL ‘avulsion’ (tearing away) injury, as we call it, can also be repaired. We use keyhole instruments to put the bone attached to the ACL back in place, and hold it there using small titanium implants. We can also use a special support to help the stability of the knee in the early phases of healing.
So, keep your ears peeled and keep yourself safe when you get back on the slopes, and have your surgeon on speed dial, so if the worst does happen you can fast track yourself an MRI.
❄ Mr Mark Frame MBChB MRCS FRSC is a trauma and knee surgeon at the University Hospital Southampton/Spire Hospital. Go to wessex-knee.com and markframe.co.uk
10th March 2020

24th March 2020
17th March 2020