Dr Frame’s Crucial Case Notes | The Dreaded ACL



This column focuses on an enthusiastic university ski racer we will call Lottie. The university race circuit is a play-hard ski-hard affair. Lottie, a qualified ski instructor and race trainer, always puts 100% into everything. This particular race was during GS training in Les Arcs. Temperatures had been warm the previous day and it had frozen overnight, leaving a hard, icy course. With the finish in sight, she straddled a gate. One ski twisted while momentum carried her forwards and downhill.
In that slow-motion moment of watching the horizon flip and spin, Lottie felt a pop. That pop was her anterior cruciate ligament. It’s a common ski injury – more so in racers as the DIN settings are high and skis will often not release, acting as a pendulum twisting your knee. As a racer you are taught to turtle and stick your feet in the air to prevent your skis getting caught and twisting if they don’t release. Watch next time you see a World Cup race on television.
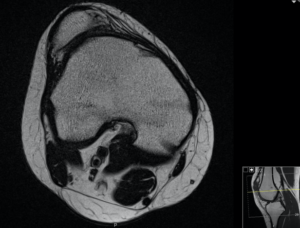
What was (not for Lottie) interesting about this ACL injury was that rather than the ligament tearing in half, it pulled off with a chunk of bone from the tibial (shin) bone side. Imagine pulling a screw from a plaster wall and rather than the screw coming out on its own you pull a chuck of plaster with it. The advantage is that bone heals well to bone and repairing the ACL rather than replacing or reconstructing it is possible. This means a quicker recovery and keeping your own important tissues rather than taking your hamstring tendons to build a new one.
In a day surgery procedure lasting less than an hour we reduced the chunk of bone back to where it had been pulled off by passing a very strong suture through the ACL. We then used a special metal button to compress the bone fragment to help it heal. To help support the healing we stabilised and took the stress off the forces through the ACL by passing an internal brace (a multi-core nylon type tape) through the fracture. Lottie was allowed to walk and weight bear normally and get her knee moving.
In six weeks she was walking without crutches. Intensive physio is crucial and after three months X-rays showed the bone fragment had healed back in. Her knee felt stable with a functioning ACL. All ready for another “enthusiastic” ski trip!
Mr Mark Frame MBChB MRCS FRSC is a trauma and knee surgeon at the University Hospital Southampton/Spire Hospital.
10th March 2020

24th March 2020
4th June 2021

